- PMID: 16429899
- PMCID: PMC1351826
Abstract
During heart transplantation, the atrial septum is most often used to reconstruct the right atrial reservoir. We report the case of a patient with corrected D-transposition of the great arteries who underwent successful cardiac transplantation despite the lack of an atrial septum. We then used the donor heart’s atrial septum for the roof of the left atrium and used the recipient’s left atrium for the back wall of the left atrium. The outcome was a more anatomically positioned transplanted heart, which avoided the duplication of the right and left atria that occurs in conventional orthotopic transplantation and that often leads to left-lower-lobe atelectasis and tricuspid regurgitation. This method of orthotopic transplantation should be considered for, but not limited to, the growing number of adults with congenital heart disease who require heart transplantation.
Keywords: Heart defects, congenital/physiopathology/surgery, heart transplantation/methods, transposition of the great vessels
The number of adult patients with congenital heart disease is approximately 800,000 in the United States alone.1 An increasing number of these patients develop systemic ventricular failure, leading to evaluation for cardiac transplantation. The literature contains few reports of heart transplantation in patients with a previous Mustard or Senning procedure.2–5 Nevertheless, because of their high late complication rates, these complex operations for transposition of the great arteries will necessitate more heart transplantation in the future.
Historically, surgeons have used the atrial septum to reconstruct the right atrial reservoir during heart transplantation. We report the case of a patient with D-transposition of the great arteries that had been corrected previously with a Mustard procedure. We performed successful transplantation despite the patient’s lack of an atrial septum. We developed a unique method of reconstruction that resulted in a more anatomically positioned transplanted heart; this method avoided the duplication of the right and left atria that occurs in conventional orthotopic transplantation and that often leads to left-lower-lobe atelectasis and tricuspid regurgitation.6
Case Report
In May 2001, a 37-year-old woman with end-stage systemic right ventricular dysfunction was evaluated for cardiac transplantation. The patient had been born with D-transposition of the great arteries. She had undergone a Blalock-Hanlon atrial septectomy during infancy and a Mustard repair with complete removal of the atrial septum at age 12 years. She was evaluated for heart transplantation and was placed on the transplant waiting list in May 2001. Thirteen months later, in June 2002, orthotopic transplantation was performed.
Surgical Technique
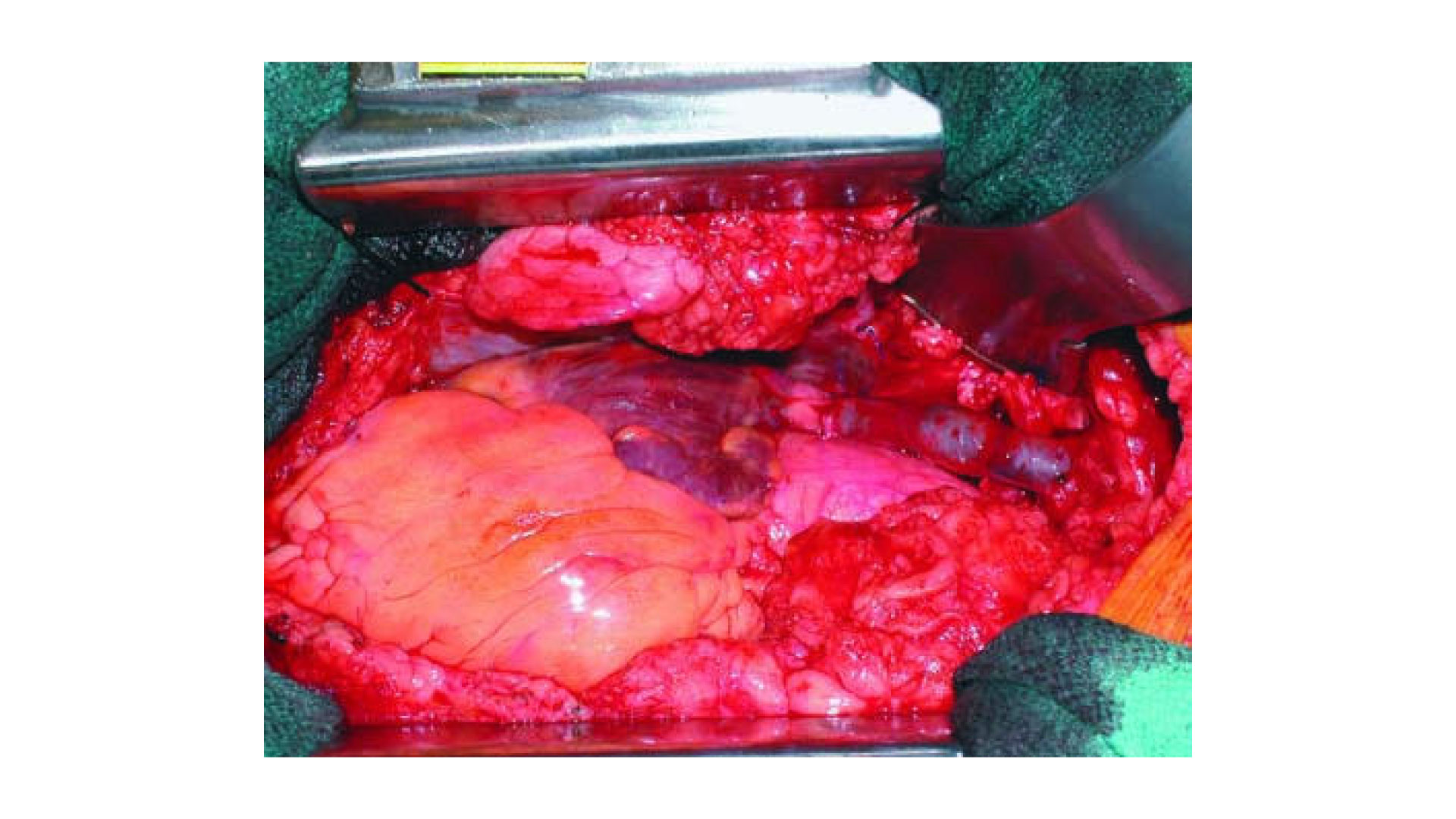
The donor heart was excised in toto, with a long length of aorta to allow for correction of the recipient’s anatomic abnormality caused by the transposition. After the native heart was also excised, we prepared the donor heart by removing the back wall of the left atrium between the entry sites of the pulmonary veins (Fig. 1A). We then anastomosed the donor heart to the recipient’s left atrium with 3-0 polypropylene sutures, beginning at the midpoint where the superior and inferior right pulmonary veins entered the donor heart (Fig. 1B). The corresponding point, located 180 opposite, was marked on the recipient’s left atrium. The donor heart was then placed in the right thoracic cavity, and the suture line was created superiorly and inferiorly to the midpoint of the left superior and inferior pulmonary veins, with a running 4-0 polypropylene suture (Fig. 1C). As this anastomosis was being completed, the donor heart was gradually transposed from its original position in the right thoracic cavity to its permanent anatomic position within the pericardial sac, in the recipient’s left thoracic cavity. The recipient’s superior and inferior venae cavae were then juxtaposed, in their normal anatomic positions, to the donor’s superior and inferior venae cavae. This maneuver enabled us to create the primary cava-to-cava anastomoses easily and rapidly (Fig. 1D). The inferior vena caval anastomosis was also performed with a running 4-0 polypropylene suture. The pulmonary artery anastomosis was constructed with 5-0 polypropylene suture, with use of bovine pericardium to reinforce the suture line. The aortic anastomosis was completed with 4-0 polypropylene suture and a strip of donor aorta (Fig. 1E). The aortic clamp was removed, and perfusion of the donor heart was initiated. After de-airing, with the donor heart beating, the superior vena caval anastomosis was created with a running 4-0 polypropylene suture, and the orthotopic transplantation was complete.

Fig. 1 A–E) Surgical technique (see text).
The patient recovered uneventfully and was easily weaned from cardiopulmonary bypass. She was discharged from the hospital 20 days postoperatively. Because of retained pacemaker leads, we were unable to perform postoperative magnetic resonance imaging; however, electrocardiographic-gated computed tomography revealed an anatomically positioned transplanted heart with a normal-sized left atrium (Fig. 2). In-travascular stents were present in the native right lower and left upper lobe pulmonary veins as a result of procedures done before transplantation. There was no evidence of pulmonary vein stenosis or misalignment. Superior and inferior venae caval drainage to the right atrium was unobstructed and appeared anatomically normal. At the last follow-up visit in June 2005, the patient was doing well and was fully ambulatory.

Fig. 2 Computed tomographic (CT) scan highlights the new technique. A) Multiplanar reconstruction in the 4-chamber projection of a contrast-enhanced multidetector CT scan. The left atrium is normal in size, and the reconstructed interatrial septum appears in the normal position. The arrow denotes a stent in the ostium of the right-upper-lobe pulmonary vein placed before transplantation. B) Three-dimensional-volume rendered reconstruction from the contrast-enhanced CT scan using a commercially available workstation (Vitrea® 2, Vital Images; Minnetonka, Minn). The left atrium (arrow) has been rendered in blue-green and isolated to allow volumetric measurements (the left atrium has a volume of 39 cc and a surface area of 85 cm2).
Comment
For most patients with congenital heart disease who undergo orthotopic heart transplantation, only minor surgical modifications are required.7 In this patient, however, the absence of an atrial septum necessitated the use of an entirely different approach to transplantation. By beginning the left atrial anastomosis on the opposite side and retaining a normal amount of left atrial tissue, we could easily perform the cava-to-cava anastomosis because the venae cavae were in a normal anatomic position. This arrangement prevented duplication of the atrial tissue, which can cause problems in positioning the heart in the left thoracic cavity. Our method is easy to perform and may also be beneficial for patients scheduled to undergo conventional orthotopic heart transplantation, because the normalized position of the left atrium prevents duplication of the right and left atrial tissue.
Footnotes
Address for reprints: O.H. Frazier, MD, Texas Heart Institute, MC 2-114A, P.O. Box 20345, Houston, TX 77225-0345
E-mail: ude.cmt.iht.traeh@nilwonk
References
Articles from Texas Heart Institute Journal are provided here courtesy of Texas Heart Institute
Orthotopic heart transplantation is a surgical procedure in which a diseased or failing heart is replaced with a healthy heart from a donor. This procedure is typically performed on patients with end-stage heart failure or severe coronary artery disease, who have not responded to other treatments. By offering a life-saving solution, orthotopic heart transplantation significantly improves both survival rates and the quality of life for patients suffering from advanced heart disease.
In this procedure, the patient’s diseased heart is removed, and a donor heart is placed in its original position in the chest cavity. The transplanted heart is then connected to the patient’s blood vessels, allowing it to take over the function of pumping blood throughout the body. One of the key benefits of orthotopic heart transplantation is its ability to restore normal cardiac function in patients whose hearts are no longer able to effectively pump blood, providing relief from symptoms such as fatigue, shortness of breath, and fluid retention.
However, orthotopic heart transplantation is not without its challenges. The need for a suitable donor heart, the risks associated with the surgical procedure, and the potential for complications such as organ rejection are important factors to consider. Patients who undergo heart transplantation must also take lifelong immunosuppressive medications to prevent rejection, which can increase the risk of infection.
Despite these challenges, orthotopic heart transplantation remains a vital treatment option for patients with end-stage heart failure, offering the opportunity for a significantly improved quality of life. Advances in surgical techniques, immunosuppressive therapy, and post-transplant care have made this procedure safer and more effective, providing hope and better outcomes for those with severe heart disease.